Acromioclavicular Joint (ACJ) Dislocation
Knowledge that empowers
What is it?
The acromioclavicular (AC) joint is comprised of the acromion (the uppermost part of the shoulder blade) and the clavicle (collarbone)
Cartilage covers each end of the joint and it is supported by a group of ligaments that provide tension across the joint which keeps the clavicle down and in line with the acromion. The joint acts as a pivot point and helps transfer load between the arm and the body.
AC joint injuries make up to 50% of all shoulder injuries. It is most often injured as a result of a fall directly onto the point of the shoulder (commonly occurs during a fall from a bike or when skiing) or a direct blow to the shoulder like a rugby tackle.
Should the force involved be great enough, the capsule and ligamentous structures that support the joint can be torn or ruptured. This results in excessive amounts of movement at the AC joint, and the two bones that form the AC joint can become separated from each other at rest or as the shoulder moves. The degree of injury can vary, depending on the force involved in the incident.
What are the symptoms?
As discussed above, AC joint arthritis can be a normal sign of ageing in the shoulder and it is not something that always causes pain or other unpleasant sensations.
A visible step deformity can sometimes be seen on the top of the shoulder in some higher grade ligament injuries as a result of the outer clavicle protrusion.
In the first few days after injury you may notice heat, swelling or bruising around the joint. Movements such as simply elevating the arm, reaching across your body, placing your hand behind your back, pushing, pulling, carrying a bag or weight bearing through your arm can be quite painful. You may not be able to lie on your shoulder and it may disturb you when you roll on it at night. As a result of pain, and a loss of the structural stability of the AC joint, your shoulder may not be as strong as normal.
How is the diagnosis made?
AC joint injury is often suspected after a traumatic injury like those mentioned previously, however it is also important to consider and rule out more serious injuries such as a clavicle or scapula fracture.
Clinical examination often reveals deformity. Examination of shoulder movement, pressing on the joint to find the specific area of tenderness and special tests that stress the AC joint help reach the diagnosis.
A specific series of plain X-rays will be ordered to determine the extent of the injury, and to exclude other injuries such as a fracture. Sometimes other investigations (like MRI) may be ordered to exclude other causes for your symptoms or associated injuries that can occur in the glenohumeral (shoulder) joint.
What is the prognosis?
AC joint injuries are typically graded by using the Rockwood classification, which describes the extent of injury to the ligaments of the AC joint and the amount of instability or separation.
Lower grade injuries often improve with time and physiotherapy, allowing you to be able to return to sport.
Some patients with higher grade injuries may do well with non-surgical treatment after the inflammation and pain settles down, although the deformity will still persist. Those patients involved in overhead sports may need surgery to restore the stability and normal biomechanics of the shoulder to allow such sporting activities.
Non surgical treatment
Initially pain relief and anti-inflammatory medication may be prescribed. Ice, rest from painful activities and a sling will also help reduce your pain.
A physiotherapist will advise you on how to best protect the healing ligaments and develop a rehabilitation programme for you. This will involve limiting activities early on that place high levels of strain on the joint, followed by progressive strengthening as symptoms settle.
Although the lower grade injuries are associated with less ligament injury, sometimes symptoms can persist for many weeks or even a number of months. In some cases if you aren’t improving as expected a corticosteroid injection into the joint may be required to help settle your pain and allow the rehabilitation to be effective.
If you are wanting to return to a contact or collision sport, you may need to wear strapping and/or padding across the AC joint. Your physiotherapist can advise you on ways to support and pad the AC joint.
Surgical treatment
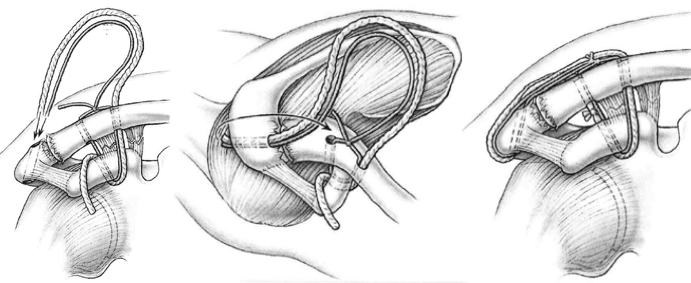
In high grade injuries or when non-surgical treatment has been unsuccessful surgery may be necessary. There are numerous types of stabilisation surgeries for the AC joint.
Most of this techniques only stabilise the AC joint in the vertical direction. Associate Professor Raniga and his Swiss colleagues have developed a novel arthroscopic (keyhole) technique that stabilises the AC joint in both vertical and horizontal directions.
After the surgery a sling is typically worn for 6 weeks and you may require some time away from work depending on what it is that you do for work.
You may commence some specific range of motion exercises during the first 6 weeks after surgery while you are in the sling. This is to maintain range of motion of the shoulder whilst also protecting any work that has been done to repair the ligaments.
After six weeks, the sling is no longer used, and exercises are commenced to restore the normal range of motion of the shoulder. Once this range of motion has been restored, strengthening exercises are commenced, along with sport or work specific rehabilitation.
You will continue to improve right up to 6 months. You will be advised on when you will be able to return to manual labour and your particular type of sport. Be sure to follow the instructions of your rehabilitation protocol and physiotherapist to ensure the best outcome after surgery.